Navigation






Rechercher

Accueil du site > Equipes de Recherche > Population, développement et environnement dans la métropole d’Accra : une étude en deux phases > Résultats
Population, développement et environnement dans la métropole d’Accra : une étude en deux phases
Résultats
 For the first phase, we began with a relatively simple model of intra-urban health patterns in Accra, hypothesizing that there was spatial variability in health within Accra and that this would be explained by the local neighbourhood environment, including the nature of the built environment (buildings and infrastructure), the socio-economic environment community and contextual factors. Our results suggest that our original hypotheses were not wrong, per se, but that the health situation in Accra is vastly more complex than the literature and thus our simpler models would suggest. Most puzzling is the relative inability of any of the usual risk factors at the individual level to explain intra-individual variability in health levels. Answers to that puzzle may lie within the neighbourhoods themselves, as suggested by the results of the geographically weighted regression. That analysis confirmed at the individual level what was shown at the ecological level. Not only do health levels vary by location within Accra, the predictors of health levels also vary according to place of residence. In particular, it is not clear whether slums are overrated or underrated with respect to their impact on health, but our analysis—the first of its kind as nearly as we can tell from the literature—indicates that slums are far from being all alike with respect to health levels. Some of the worst slums in Accra also have some of the poorest health levels, but some do not. Furthermore, poor health is evident in some places that are not considered to be slums, and some slum areas have reasonably good levels of health. The contribution of non-random sorting using ethnicity was explored in depth and published in Urban Geography (2006).
For the first phase, we began with a relatively simple model of intra-urban health patterns in Accra, hypothesizing that there was spatial variability in health within Accra and that this would be explained by the local neighbourhood environment, including the nature of the built environment (buildings and infrastructure), the socio-economic environment community and contextual factors. Our results suggest that our original hypotheses were not wrong, per se, but that the health situation in Accra is vastly more complex than the literature and thus our simpler models would suggest. Most puzzling is the relative inability of any of the usual risk factors at the individual level to explain intra-individual variability in health levels. Answers to that puzzle may lie within the neighbourhoods themselves, as suggested by the results of the geographically weighted regression. That analysis confirmed at the individual level what was shown at the ecological level. Not only do health levels vary by location within Accra, the predictors of health levels also vary according to place of residence. In particular, it is not clear whether slums are overrated or underrated with respect to their impact on health, but our analysis—the first of its kind as nearly as we can tell from the literature—indicates that slums are far from being all alike with respect to health levels. Some of the worst slums in Accra also have some of the poorest health levels, but some do not. Furthermore, poor health is evident in some places that are not considered to be slums, and some slum areas have reasonably good levels of health. The contribution of non-random sorting using ethnicity was explored in depth and published in Urban Geography (2006).
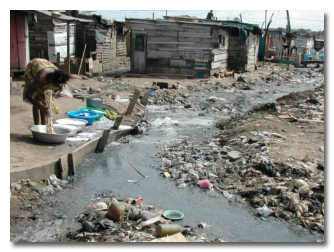
 One technical problem involves the measurement of the health outcomes of interest. In most previous studies, self-rated health was chosen as the dependent variable. Our work and others associated with the WHO World Health Survey have shown the importance of cut-points in these assessments, which are themselves associated with social class. Thus, we often find an inversion of the usual gradient in health by social class with the poorest or lowest SES group reporting the lowest morbidity. An additional technical dimension in the objectively assessed health measures we were able to obtain in the Women’s Health Survey was that the pattern of morbidity varied widely by SES. Thus, we found that the poor, especially those living in low lying areas by the river, were more prone to infectious conditions (malaria in particular) whereas the higher social class were more afflicted by chronic conditions such as the risk factors for cardio-vascular disease. This complicates the comparison of even objectively assessed health states by social class.
One technical problem involves the measurement of the health outcomes of interest. In most previous studies, self-rated health was chosen as the dependent variable. Our work and others associated with the WHO World Health Survey have shown the importance of cut-points in these assessments, which are themselves associated with social class. Thus, we often find an inversion of the usual gradient in health by social class with the poorest or lowest SES group reporting the lowest morbidity. An additional technical dimension in the objectively assessed health measures we were able to obtain in the Women’s Health Survey was that the pattern of morbidity varied widely by SES. Thus, we found that the poor, especially those living in low lying areas by the river, were more prone to infectious conditions (malaria in particular) whereas the higher social class were more afflicted by chronic conditions such as the risk factors for cardio-vascular disease. This complicates the comparison of even objectively assessed health states by social class.
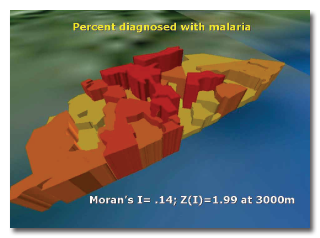
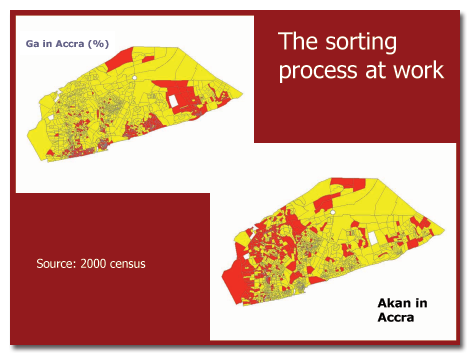 Overall, we do see clustering of health conditions by district although these district level effects cannot be readily distinguished from some historical patterns of ethnic concentration in the city. The Ga, the oldest established residents of Accra, are concentrated in some former villages – Jamestown, Osu, La – now absorbed into the city and at the same time these older neighbourhoods share common characteristics such as crowding, proximity to the sea and an older housing fabric.
Overall, we do see clustering of health conditions by district although these district level effects cannot be readily distinguished from some historical patterns of ethnic concentration in the city. The Ga, the oldest established residents of Accra, are concentrated in some former villages – Jamestown, Osu, La – now absorbed into the city and at the same time these older neighbourhoods share common characteristics such as crowding, proximity to the sea and an older housing fabric.
The key results of the second phase can be summarized as follows. The responses suggest that the people interviewed perceive environmental pollution as the major source of environmental risks in Nima and Maamobi. On the whole, the environmental risks are more pronounced in Maamobi than Nima. Flooding, environmental pollution, unapproved settlement patterns, animal husbandry and disregard for institutional regulations are the major environmental risks in Maamobi. These situations are closely related to the relatively low educational levels in Maamobi. In Nima where the educational levels are relatively higher, similar environmental risks are relatively low. It would seem that these responses suggest more exposure to environmental risks in Maamobi than in Nima. The severity of these environmental risks in the two communities is important. The study therefore assessed the degree of the environmental risks in terms of their severity in the two communities. The major causes of environmental risks in Nima and Maamobi are many and varied. These various causes are stated under each environmental risk in relation to the responses from Nima and Maamobi.
There seems to be no significant difference between Nima and Maamobi with regard to the causes of environmental risks. Poor drainage, choked gutters, solid waste disposal, liquid waste disposal, choked and stinking drains and low income among others are relatively high in both communities. It does not seem easy to explain away the variations of the causes of environmental risks in terms of the relative level of literacy or ethnicity in both communities. Overcrowding and high room occupancy ratios are higher in Nima than Maamobi despite the fact that literacy rates are relatively higher in Nima than Maamobi. The level of responses to the causes of environmental risks in both communities suggests that they are indeed very poor urban neighbourhoods. Opinions in the two communities vary on the role the central government should play in coping with the environmental risks and health problems. In Nima, law enforcement, provision of refuse containers and intensive public education featured prominently in the opinions expressed on the central government’s role in coping with environmental risks and health problems. In Maamobi, law enforcement, provision of more public toilets and provision of logistic support for communal labour are important roles that the Central Government should play in coping with environmental risks and health problems in their community.
The detailed work in Nima-Maamobi also brought out some clear differences in community responsibility even between these two low income areas. In Nima, more homogenous and consisting of migrants from the north, the willingness to engage in communal efforts to improve health seemed more developed. Encouragement of communal labour especially in Nima, adherence to public regulations and public education on sanitation especially in Maamobi are the major opinions expressed by the communities in Nima and Maamobi on the roles the communities should play to cope with the environmental risks and health problems.
An additional variable leading to the development of social networks and associations may be the duration of residence of migrants and residents in particular neighbourhoods. The debate on the significance of social capital – social arrangement and functions operating at a level beyond the aggregate of individual actions – is still raging and unfortunately our data are not dense enough on the Nima-Maamobi case to decide if there are additional over-arching social functions that go beyond kinship ties or the participation of individuals in clubs and associations to maximize individual rather then collective gain. This work will probably need to adopt a more long term anthropological approach to such issues.
Access to the remotely sensed data added some additional truly ecological variables to the analysis. At the local level, people’s perception of environmental risk was not necessarily adapted to the public health risk factors commonly linked to the infectious conditions – malaria, diarrhoea and cholera, for example. Although rubbish in the streets is a nuisance, attracting rodents and other pests, very few rated the introduction of latrines or piped sewage above other possible sanitary improvements.